Inherited breast cancer is rare and causes only 5% of all breast cancers. Yet it is one of the major reasons of concern for many women who have experienced breast or ovarian cancer because it affected their mums, sisters or aunts. Genetic risk for breast cancer is one of the factors that you can’t modify, but it can be a lifesaver in many ways. During Women’s Health Month, Professor Zoe Winters, Breast Surgeon at New Victoria Hospital, explains why genetic testing is becoming mainstream as an essential tool for prevention as well as for more successful treatment outcomes.
What is the genetic risk for breast cancer?
The genetic risk for some types of cancers lies in the mutation of certain genes that can be inherited from both parents and considerably raise the risk for breast cancer and other types of cancer, such as ovarian and possibly prostate, pancreatic, colon, stomach, thyroid and uterine cancers .
Inherited gene mutations, also called germline alterations, can predict a high lifetime risk ranging from 35 to 80% by 80 years of age.
The two most common inherited gene mutations are BRCA1 and BRCA2 and a gene called PALB2.
Mutations or abnormal function of the BRCA1/2 genes means that cancer cells cannot detect damages to their genetic material or DNA and cannot repair their damaged DNA. This is why cancers occur at such high rates in these patients.
A positive BRCA1 result gives a woman a 60% to 80% lifetime risk of breast cancer and a 30% to 45% lifetime risk of ovarian cancer. A positive BRCA2 result gives a woman a 50% to 70% lifetime risk of breast cancer and a 10% to 20% lifetime risk of ovarian cancer.
Breast health and genetic testing
Genetic testing is useful both as a form of prevention, called a predictive genetic test, or to make informed decisions on therapy paths to follow if you are diagnosed with breast cancer.
Predictive genetic testing can either give you peace of mind if mutations are not present or help you take action should your result come back positive.
Having gene mutations increases the risk of developing breast cancer, but it doesn’t mean that you have it or will certainly develop it.
If you do have gene mutations, your Consultant will go through all the available options with you so that you can make an informed choice when it comes to breast cancer prevention.
You might want to consider surgery and have your breasts removed. Alternatively, you might want to go for a screening once a year, knowing that your risk of developing breast or ovarian cancer is higher due to the gene mutation.
What genes do molecular tests include?
Currently, the guidelines for testing high-risk genes have expanded with lowered thresholds for genetic testing of the following genes:
- BRCA1
- BRCA2
- PALB2
- CHD1
- P53
- PTEN
- ATM
- CHEK2
Who should have a molecular genetic test?
It is advisable to have a genetic test if you:
- Have a relative who has tested positive for a genetic mutation
- Have a strong family history for any type of cancer, in particular, prostate, pancreatic, colonic, stomach, thyroid, and uterine cancer, amongst others
- Have a personal history of cancer
One-Stop Breast Clinic and genetic testing
The One-Stop Breast Clinic at New Victoria Hospital offers an efficient screening for all patients who want to have a specialist consult with a highly experienced Breast Surgeon.
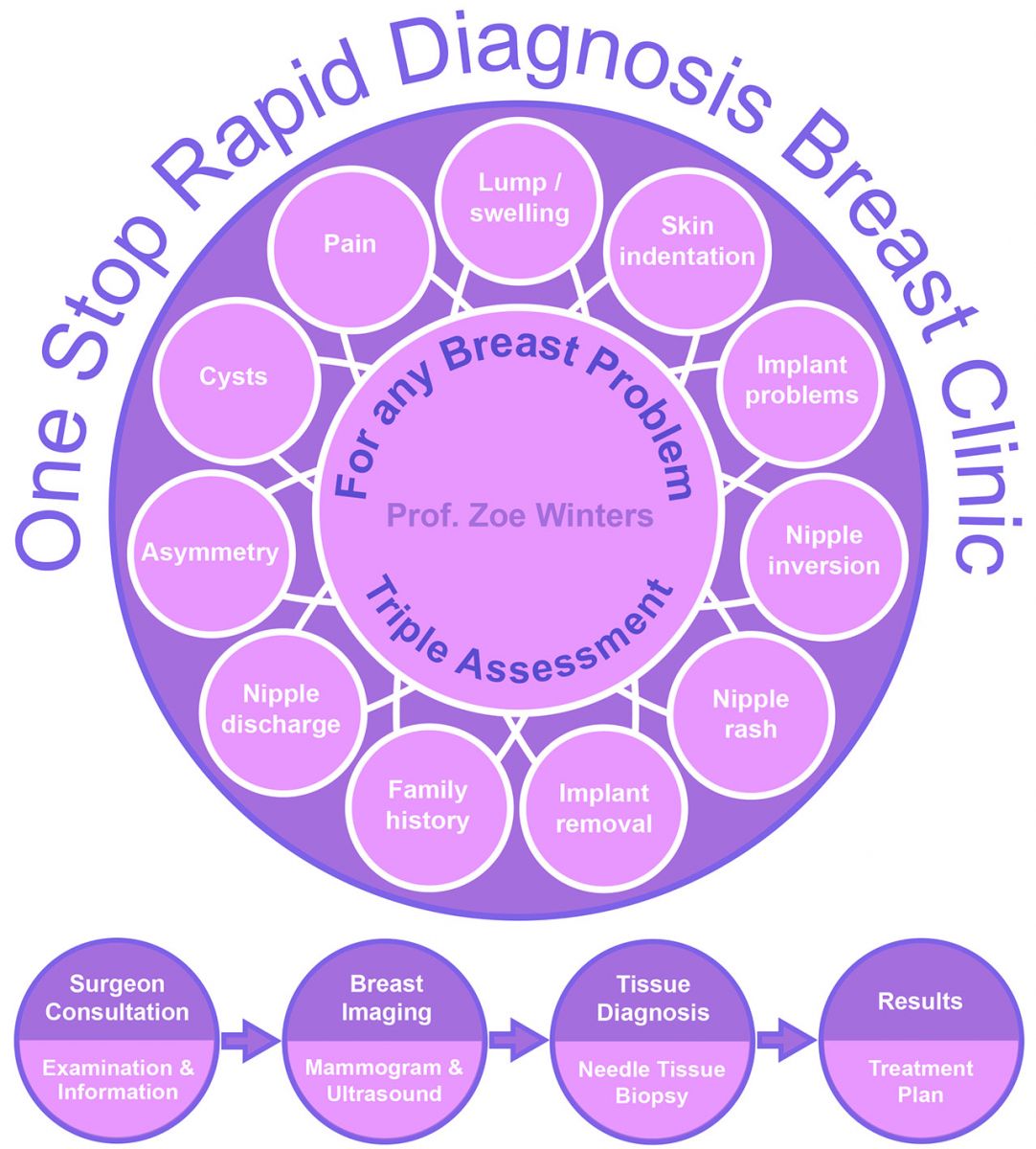
After your consultation, you can be quickly referred for diagnostic Imaging examinations and have a biopsy done, in most cases on the same day, with results provided within 48-72 hours.
Genetic testing at our One-Stop Breast Clinic
During your consultation, you will receive appropriate information regarding genetic risk for breast cancer.
If you have a relative who tested positive for gene alterations or a family history of any cancer, your Breast Surgeon will advise you to see a Consultant Geneticist and can facilitate your referral.
Genetic testing is a valuable tool in treatment decision-making for both early and advanced-stage breast cancer.
It helps your consultant and you to make informed decisions on the most effective treatments after breast cancer is diagnosed or after breast surgery.
The Oncotype DX Breast Recurrence Score Test, for instance, analyses the activity of a 21 group of genes that can affect how early-stage breast cancer is likely to behave and respond to treatment. The test can be a good predictor of potential distant recurrence, which happens when the oestrogen-receptor positive breast cancer comes back in a different part of the body, and also how the tumour will respond to chemotherapy.
The results of the Oncotype DX Breast Recurrence Score Test, combined with other features of the cancer, can help you make a more informed decision about whether or not to have chemotherapy to treat early-stage, hormone-receptor-positive, HER2-negative breast cancer.
The genetic deficiency can be used as a treatment advantage when combined with drugs that block sensors of DNA damage and repair. These drugs are called PARP inhibitors, and they effectively kill BRCA1/2 abnormal cancer cells where the BRCA genes aren’t functioning. The PARP inhibitors sensitise BRCA cancers to the DNA damaging effects of chemotherapy and radiotherapy.
The platinum types of chemotherapy, like Carboplatin, an intravenous drug, are also particularly effective in killing BRCA mutated breast cancers.
These drugs are also highly effective in treating triple negative breast cancers – with no expression of oestrogen, progesterone or the HER2 gene- that carry mutations of the BRCA1 (70%) or BRCA2 (20%) genes.
The more recent testing of the PALB2 gene (Partner and Localizer of Breast Cancer 2 (BRCA2)) functions together with the BRCA2 gene and serves as an additional drug able target for cancer treatments.
All women previously undergoing BRCA testing before 2014 should be referred for retesting of BRCA1/2 and PALB2.
Women with advanced breast cancer that carried BRCA mutations were treated with PARP inhibitors in two breast cancer trials called OLYMPIAD and EMBRACA.
They both showed a significant improvement in cancer-free survival.
Currently, there are many breast cancer trials evaluating PARP inhibitors either at the pre-surgery (neoadjuvant) or post-surgery (adjuvant) stages of treatments in women with BRCA abnormal genes.
Another method to identify gene expressions, using messenger RNA, called transcriptome profile, provides us with much more prognostic/predictive information on the full spectrum of breast cancers over and above routine breast cancer staging.
These tests can identify those women who will benefit from chemotherapy after surgery and allows us to recommend personalised treatments where chemotherapy may not be required.
Results from other studies show greater benefits of chemotherapy in addition to ER+ endocrine treatment in younger women compared to those >50 years.
Molecular testing of breast cancer is a rapidly evolving field and is here to stay!
If you are concerned about genetic risk factor for breast cancer, you can book an appointment with our Consultant Breast Surgeons at New Victoria Hospital’s One-Stop Breast Clinic by calling us on 020 8949 9020 or: